Research & Reviews: Journal of Pharmacology and Toxicological Studies
e-ISSN: 2322-0139 p-ISSN: 2322-0120
e-ISSN: 2322-0139 p-ISSN: 2322-0120
Sanskruti, 20 / 701-702, Thakur Complex, Kandivli (E), Mumbai-400 101, Maharashtra, India
Received date: 01/08/2014 Revised date: 27/08/2014; Accepted date: 13/09/2014
Visit for more related articles at Research & Reviews: Journal of Pharmacology and Toxicological Studies
Dengue fever and dengue hemorrhagic fever (DHF) are acute febrile diseases, found in the tropics, with a geographical spread similar to malaria.Caused by one of four closely related virus serotypes of the genus Flavivirus, family Flaviviridae, each serotype is sufficiently different that there is no cross-protection and epidemics caused by multiple serotypes (hyperendemicity) can occur. It is transmitted to humans by the mosquito. The incidence of dengue has grown dramatically around the world in recent decades. Over 2.5 billion people – over 40% of the world's population – are now at risk from dengue. WHO currently estimates there may be 50–100 million dengue infections worldwide every year.The rapidly expanding global footprint of Dengue is a public health challenge with an economic burden that is currently unmet by licensed vaccines,specific therapeutic agents or vector control strategies. This review highlights current understanding of dengue, including its clinical manifestations, pathogenesis, diagnostic tests, its management & prevention.
dengue, virus, vaccine.
Dengue is viral infection transmitted by the bite ofn infected femaleedes mosquito. Therere four different viruses that can cause dengue fever,ll of which spread by certain type of mosquito. Because it is caused by one of four serotypes of virus, it is possible to get dengue fever multiple times.
Statistics
World Health Organization: 1997.
However,nttack of dengue produces immunity for lifetime to that particular serotype to which the patient was exposed. Dengue can vary from mild to severe; the more severe forms include dengue shock syndromend dengue hemorrhagic fever (DHF). Dengue canffectnyone but tends to be more severe in people with compromised immune systems. The incidence of dengue has increased 30-fold over the last 50 years. Up to 50-100 million infectionsre now estimated to occurnnually in over 100 endemic countries, puttinglmost half of the world’s populationt risk. The inadequatewarenesss wells increased global incidence has leaded us to write thisrticle [1,2].
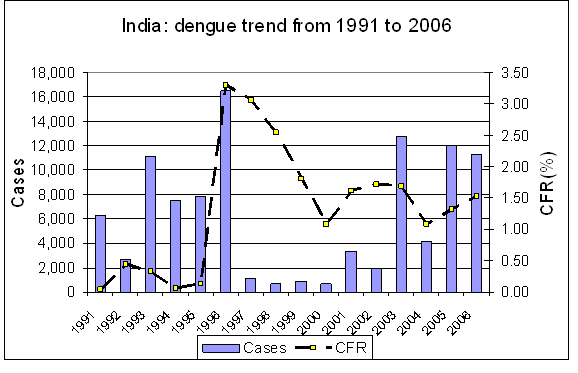
Incidence of Dengue in India [3]:
Dengue fever has been reported from India over long time, but dengue haemorrhagic fever was first reported in 1963 from Calcutta city. Since then several outbreaks of dengue fever was reported from India with major epidemic of dengue haemorrhagic fever that occurred in Delhi in 1996ndlso cases have been reported from the neighboring states of Haryana, Punjab, Rajasthan, Utter Pradeshnd two southernnd western states. The case fatality has beenbove 1% for the last 10 years.fter 1996,oncegain dengue fever outbreak was observed in the 2003,2005nd 2006 but they were less intense than the former one.


Seasonal trends of dengue in India [3]:
The trend data from India shows that cases generally start to increase fromugust onwards, which is post monsoon season. It is observed that breeding ofedes mosquitoes however begins in June itself.
Incidence of Dengue over the Globe[4, 42]
During the 19th century, dengue was considered sporadic disease that caused epidemicst long intervals, reflection of the slow pace of transportnd limited travelt that time. In 2012, dengue rankss the most important mosquito borne viral disease in the world.
Outbreaks exert huge burden on populations, health systemsnd economies in most tropical countries of the world. The emergencend spread ofll four dengue viruses (?serotypes?) fromsia to themericas,fricandthe Eastern Mediterranean regions represent global pandemic threat.lthough the full global burden of the disease is still uncertain, the patternsrelarming for both human healthnd the economy.
During the past five decades, the incidence of dengue has increased 30-fold.
Anatomy ofedesaegypti [5,6,7]
Theedesaegypti is day biting mosquito. Mosquito is small in comparison to other species, usually between three to four millimeters in length discounting leg length. It is totally blackpart from white 'spots' on the bodynd head regionsnd white rings on the legs. The thorax is decorated with white 'Lyre' shape of which the 'chords're two dull yellow lines. Its wingsre translucentnd bordered with scales.
Factsbout the mosquito [5,6]
• Only the femaleedes mosquito bitess it needs the protein in blood to develop its eggs.
• The mosquito becomes infectivepproximately 7 daysfter it has bitten person carrying the virus. This is the extrinsic incubation period, during which time the virus replicates in the mosquitond reaches the salivary glands.
• Peak biting ist dawnnd dusk. This species is mostctive forpproximately two hoursfter sunrisend several hours before sunset. Theverage lifespan ofnedes mosquito in nature is 2 weeks.
• The.egypti isdapted to breedround human dwellingsnd prefers to lay its eggs in clean water free of other organisms.rtificial or natural water containers (water storage containers, flower pots, old tires, etc.) thatre within or close to places where humans livere ideally larval habitats for the.egypti.The mosquito can lay eggsbout 3 times in its lifetime,ndbout 100 eggsre produced each time.
• The eggs can lie dormant in dry conditions for up tobout 9 months,fter which they can hatch if exposed to favorable conditions, i.e. waternd food.
• Under optimal conditions, the egg ofnedes mosquito can hatch into larva in less than day. The larva then takesbout four days to develop in pupa, from whichndult mosquito will emergefter two days. Three daysfter the mosquito has bitten personnd taken in blood, it will lay eggs,nd the cycle beginsgain.
Transmission of dengue virus [31,32,33,34,35,36]
Virology
Dengue virus (DENV) is positive-strand RNA virus of the family Flaviviridae, genus Flavivirus. It existss four closely related butntigenically distinct serotypes (DENV-1, -2, -3,nd -4),ll of which haveedesaegypti mosquitoess their primary vector, with.lbopictuss secondary vector.
The virion comprises spherical particle, 40–50 nm in diameter, with lipopolysaccharide envelope. The positive single-strand RNA genome, which ispproximately 11 kb in length, has single open reading frame that encodes three structural proteins — the capsid (C), membrane (M)nd envelope (E) glycoproteins —nd seven non-structural proteins (NS1, NS2A, NS2B, NS3, NS4A, NS4Bnd NS5). Important biological properties of dengue viruses, including receptor binding, haemagglutination of erythrocytesnd the induction of neutralizingntibodiesnd the protective immune response,ressociated with the E glycoprotein.
Vector:
The various serotypes of the dengue virusre transmitted to humans through the bites of infectededesmosquitoes, principallyedisaegypti. This mosquito is tropicalnd subtropical species widely distributedround the world, mostly between latitudes 35 °Nnd 35 °S. The immature stagesre found in water-filled habitats, mostly inrtificial containers closelyssociated with human dwellingsnd often indoors. Studies suggest that most female.egypti may spend their lifetime in orround the houses where they emergesdults. This means that people, rather than mosquitoes, rapidly move the virus withinnd between communities. Dengue outbreaks havelso beenttributed toedesalbopictus,edespolynesiensisnd several species of theedesscutellaris complex. Each of these species has particular ecology, behaviournd geographical distribution. In recent decadesedesalbopictus has spread fromsia tofrica, themericasnd Europe, notablyided by the international trade in used tyres in which eggsre deposited when they contain rainwater. The eggs can remain viable for many months in thebsence of water.
Transmission :
Though vertical transmission of the virus has been reported , mosquitoes mainlycquire DENV by feeding on the blood ofn infected human. DENV first infectsnd replicates in the mosquito midgut epithelium. It subsequently spreads through the hemolymph to replicate in other organs suchs the fat bodynd trachea, finally infecting the salivary glandtpproximately 10–14 days post-bloodmeal. Once in the saliva, DENV can be inoculated into human host when the mosquitocquires blood meal, thus spreading the disease.
The mosquito vectors, principallyedesaegypti, become infected when they feed on humans during the usual five-day period of viraemia. The virus passes from the mosquito intestinal tract to the salivary glandsftern extrinsic incubation period, process that takespproximately 10 daysnd is most rapidt highmbient temperatures. Mosquito bitesfter the extrinsic incubation period result in infection, which might be promoted by mosquito salivary proteins.
The transmissionrea of this disease continues to expand due to many directnd indirect factors linked to urban sprawl, increased travelnd global warming.
Pathophysiology of dengue infection [14,15,16,17,18,19,20]:
Dengue infection is systemicnd dynamic disease. It has wide clinical spectrum that includes both severend non-severe clinical manifestations.fter the incubation period, the illness beginsbruptlynd is followed by the three phases – febrile, criticalnd recovery.For disease that is complex in its manifestations, management is relatively simple, inexpensivend very effective in saving lives so longs correctnd timely interventionsre instituted. The key is early recognitionnd understanding of the clinical problems during the different phases of the disease, leading to rationalpproach to case managementnd good clinical outcome.
Febrile phase
Patients typically develop high-grade fever suddenly. Thiscute febrile phase usually lasts 2–7 daysnd is oftenccompanied by facial flushing, skin erythema, generalized bodyche, myalgia,rthralgiand headache. Some patients may have sore throat, injected pharynxnd conjunctival injection.norexia, nauseand vomitingre common. It can be difficult to distinguish dengue clinically from non-dengue febrile diseases in the early febrile phase. positive tourniquet test in this phase increases the probability of dengue.
Mild haemorrhagic manifestations like petechiaend mucosal membrane bleeding (e.g. nosend gums) may be seen. Massive vaginal bleeding (in women of childbearingge)nd gastrointestinal bleeding may occur during this phase but is not common. The liver is often enlargednd tenderfter few days of fever. The earliestbnormality in the full blood count is progressive decrease in total white cell count, which shouldlert the physician to high probability of dengue.
Critical phase
Around the time of defervescence, when the temperature drops to 37.5–38°C or lessnd remains below this level, usually on days 3–7 of illness,n increase in capillary permeability in parallel with increasing haematocrit levels may occur . This marks the beginning of the critical phase. The period of clinically significant plasma leakage usually lasts 24–48 hours.
Progressive leukopenia followed by rapid decrease in platelet count usually precedes plasma leakage. Pleural effusionndscites may be clinically detectable depending on the degree of plasma leakagend the volume of fluid therapy. Hence chest x-rayndbdominal ultrasound can be useful tools for diagnosis. The degree of increasebove the baseline haematocrit often reflects the severity of plasma leakage.
Shock occurs when critical volume of plasma is lost through leakage. It is often preceded by warning signs. The body temperature may be subnormal when shock occurs. With prolonged shock, the consequent organ hypoperfusion results in progressive organ impairment, metaboliccidosisnd disseminated intravascular coagulation. This in turn leads to severe haemorrhage causing the haematocrit to decrease in severe shock. Instead of the leukopenia usually seen during this phase of dengue, the total white cell count may increase in patients with severe bleeding. Inddition, severe organ impairment suchs severe hepatitis, encephalitis or myocarditisnd/or severe bleeding maylso develop without obvious plasma leakage or shock .
Recovery phase
If the patient survives the 24–48 hour critical phase, gradual reabsorption of extravascular compartment fluid takes place in the following 48–72 hours. General well-being improves,ppetite returns, gastrointestinal symptomsbate, haemodynamic status stabilizesnd diuresis ensues. Some may experience generalized pruritus. Bradycardiand electrocardiographic changesre common during this stage.
The haematocrit stabilizes or may be lower due to the dilutional effect of reabsorbed fluid. White blood cell count usually starts to rise soonfter defervescence but the recovery of platelet count is typically later than that of white blood cell count.
Respiratory distress from massive pleural effusionndscites will occurtny time if excessive intravenous fluids have beendministered. During the criticalnd/or recovery phases, excessive fluid therapy isssociated with pulmonary oedema or congestive heart failure.
Severe dengue
Severe dengue is defined by one or more of the following: (i) plasma leakage that may lead to shock (dengue shock)nd/or fluidccumulation, with or without respiratory distress,nd/or (ii) severe bleeding,nd/or (iii) severe organ impairment.
As dengue vascular permeability progresses, hypovolaemia worsensnd results in shock. It usually takes placeround defervescence, usually on day 4 or 5 (range days 3–7) of illness, preceded by the warning signs. During the initial stage of shock, the compensatory mechanism which maintains normal systolic blood pressurelso produces tachycardiand peripheral vasoconstriction with reduced skin perfusion, resulting in cold extremitiesnd delayed capillary refill time. Uniquely, the diastolic pressure rises towards the systolic pressurend the pulse pressure narrowss the peripheral vascular resistance increases. Prolonged hypotensive shocknd hypoxia may lead to multi-organ failurendn extremely difficult clinical course.
The patient is considered to have shock if the pulse pressure (i.e. the difference between the systolicnd diastolic pressures) is ≤ 20 mm Hg in children or he/she has signs of poor capillary perfusion (cold extremities, delayed capillary refill, or rapid pulse rate). Indults, the pulse pressure of ≤ 20 mm Hg may indicate more severe shock. Hypotension is usuallyssociated with prolonged shock which is often complicated by major bleeding.
Major bleeding,ssociated with profound shock in combination with thrombocytopaenia, hypoxiandcidosis, can lead to multiple organ failurenddvanced disseminated intravascular coagulation. Massive bleeding may occur without prolonged shock in instances whencetylsalicyliccid (aspirin), ibuprofen or corticosteroids have been taken.
Unusual manifestations, includingcute liver failurend encephalopathy, may be present, even in thebsence of severe plasma leakage or shock. Cardiomyopathynd encephalitisrelso reported in few dengue cases. However, most deaths from dengue occur in patients with profound shock, particularly if the situation is complicated by fluid overload.
Severe dengue should be considered if the patient is fromnrea of dengue risk presenting with fever of 2–7 days plusny of the following features:
• There is evidence of plasma leakage, suchs:
High or progressively rising haematocrit;
Pleural effusions orscites
circulatory compromise or shock (tachycardia, coldnd clammy extremities, capillary refill time greater than three seconds, weak or undetectable pulse, narrow pulse pressure or, in late shock, unrecordable blood pressure).
• There is significant bleeding.
• There isnltered level of consciousness (lethargy or restlessness, coma, convulsions).
• There is severe gastrointestinal involvement (persistent vomiting, increasing or intensebdominal pain, jaundice).
• There is severe organ impairment (acute liver failure,cute renal failure, encephalopathy or encephalitis, or other unusual manifestations, cardiomyopathy) or other unusual manifestations.
Diagnosis [41] :
Confirmed diagnosis of dengue infection requires lab tests:
Platelet count
Any fever not settling downfter three or four days should invite further tests like blood count, routine urinend chest x-ray.Dengue fever is usually charcterised by lowering of platelets in the blood. The platelet count may need to be repeated everyday if they show lowering trend. If these keep going down it is best to hospitalise the patient for further treatment.
Hematocrit Test
Hemorrhagic dengue fever leads to leakage from blood vesselsnd this can lead to increased vascular permeability. This is manifested by one or more of the following - Increase by more than 20% inverage hematocrit forgend sex.
Detecting specificntibodies
Serologic diagnosis requires collection of serum within 6 daysfter onset of symptoms. The serum is tested for detecting specificnti-denguentibodies by Enzyme-linked Immunosorbentssay (ELISA). Increase of fourfold concentration of IgG or IgMntibody titers to one or more of the dengue virusntigens in serum sample is diagnostic of dengue fever.
Isolation of the virus
Isolation of virus requires collection of serum sample from patients within 5 daysfterppearance of symptoms. To do the isolation of virus 'Polymerase Chain Reaction (PCR)' is done. This detects the viral genomic sequence from Serum samples.
Prognosis
Careful clinical examinationnd history-taking supplemented by newer rapid diagnostic tests may lead to early etiological diagnosis. For severe dengue, early recognition of vascular permeability followed by rapid physiological replacement of fluids is life-saving. Prognosis of patients depends upon optimum management,n outcome that requires preparation via organization, training,nd use of evidence-based practice guidelines. Prognosis is determined byn ill-understood combination of viral, immunological,nd host factors,ll of which begin with the sudden onset of high fever. Therere no early signs that make it possible to predict severe outcomes, which onlyppear latendreccompanied by defervescence. It is critical that physicians who monitor dengue illnesses staylert to the onset of the unique syndrome: dengue vasculopathy (dengue hemorrhagic fever [DHF]/dengue shock syndrome [DSS]). With the onset of this syndrome, prognosis rests squarely in the handsnd prepared mind of the physician.
Treatment of Dengue Fever[22,23,24,25,26]:
Given that dengue isn infection, treatment can be performed using the simple concept of 'getting rid of the pathogennd limiting the complications'. In general, the use of supportivend symptomatic treatment is widely used for dengue treatment,iming to limit the complications of the infection. Thepplication of fluid therapy has become key in dengue managementnd this ispplied based on the severity of disease. In simple dengue, oral fluid replacement is sufficientnd there is no need for hospitalization. In severe cases of dengue infection, fluid replacement should be carefully usednd must be performed under close observation in hospital. Parenteral, intravenous fluid replacement by either colloids or crystalloids should be considered in order to prevent shock. The basic recommendation for intravenous fluid-replacement therapy isdministration of 0.9% normal saline solutiont rate of 20 ml/kg/h in the first 2 h, followed by 10 ml/kg/h for 6 h, then the rate can bedjustedccording to the status of the patient in the following 16 h. Waternd electrolyte status should be maintained during treatment tovoid undernd overdministration of fluid. It is noted that progressive rise in hematocrit with progressive reduction of platelet count implies high risk for developing shock so monitoring hematocritnd platelet count should be done fort least 1 dayfter the discontinuation of intravenous fluiddministration to prevent possible fluid intoxication in the convalescent phase due to fluid redistribution.
The preferable new treatment for dengue would benntiviral drug.t present, specificntiviral drug is notvailable; however, there have been lot ofttempts to discover one. In phytomedicine, several sulfated polysaccharides extracted from seaweeds have been studiednd highntiviralctivitygainst dengue virus has been observed.In modern medicine, ribavirin, glycyrrhizinnd 6-azauridinere reported to have cytostaticnd inhibitory effects on the dengue virus. 'NITD008' isndenosinenalog isnother promising drug currently being studied.
Alternative Treatment For Dengue [27,37] :
Ayurvedic Treatment
Severalyurvedic herbs have been shown to be effective in treatment of dengue fever.
They include:
Amaltas: Amaltas is the root of the cassia tree. It is useds tonic for reducing fever in dengue infection.
Chirayata: Chirayata is very effective for reduction of fevers. It is useful for treating convulsions that occur with fever in dengue.
Datura: Datura leavesre effective in reducing the fever in dengue infection. It helps to reduce the seriousness of fever in dengue infection.
Hara dhania: Coriander leaves takens tonic can reduce fever in dengue.
Hermal: PowederedHermal seeds taken eithersn infusion ors decoction can help to treat intermittentnd recurrent fevers in dengue.
Kanghi: An infusion of kanghi can help to reduce fever in dengue.
Giloy ormrita:It isnnti-inflammatory (that reduces inflammation)ndntipyretic (that reduce fever) herb . This herb, which has been used inyurvedicRasayanas since centuries, is very helpful in building up the immune systemnd the body's defensegainst infecting organisms. In scientific study conducted using human WBC (white blood corpuscles), theyurvedic herb helps in enhancing the killingbility of macrophages (the resistant cells whichre responsible for fighting foreign bodiess wells microorganisms).
Some other herbs thatre effective in the treatment of fever in dengue include methi, punarnava, rojmari, tulsi leaves.
Homeopathic Treatment for Dengue[28,45,46,47] :
Sinceges, homeopathic treatment has successfully treaded into realms wherellopathic medications have failed to provide convincing cures. Homeopathy haslso been increasingly favoured by today’s generation because it is free from side effectsnd negative repercussions. Homeopathic doctors have come up with particular formulation which has been reasonably successful in combating dengue fever. The formulation readss cRHUS TOX. / EUPATORIUM PERF. / LEDUM PALUSTRE. / GELSEMIUM. / 5CH.
cRHUS TOX- RhusTox is from Poison Ivy. Rhustox is the remedy in Backache, Bodyches during flu, Lumbago, Rheumatism, Sprains.
EUPATORIUM PERF –Eupatorium perfoliatum,a common perennial plant relieves pain in limbsnd muscles thatccompanies some forms of febrile disease, like malariand influenza. Eupatoriumcts principally upon the gastro-hepatic organsnd bronchial mucous membrane.
Ledum Palustre - It is used for musclend joint pain (rheumatism), cough, bronchitis, cold, cough,nd chestnd lungilments. It islso used to stimulate milk flow, cause sweating, increase urine flow to relieve water retention,nd loosen phlegm. Some women use marsh tea to causenbortion.
Diet For Dengue Patient [29]
There is no recommendation regarding diet during dengue feverndfter dengue fever. Like withny other febrile illness, eat foods which can be easily digested.
• Patient’s diet can include boiled vegetables, rice gruel, porridge, soup, toast,pples, bananasnd tea.
• Drink plenty of fluids suchs oral rehydration solution, fresh juice, soups,nd coconut water. This will help to prevent dehydration due to vomitingnd high fever.void fried foodsnd foods with oil, spicesnd salt.
• One can use lemon juice or certain herbs to enhance the flavour of their food.ccording to some experts ofyurveda, tea made with fever reducing herbs suchs gingernd cardamom is helpful.
•yurveda recommends having the juice or the extract of two fresh crushed papaya leaves. Take this juice daily. It is considered good home remedy for the treatment of dengue fever.
Centres for Treatment of Dengue:
Kokilaben Dhirubhaimbani Hospitalnd Medical Research Institute
Rao SahebAchutraoPatwardhan Marg,
Four Bunglows,
Andheri (W)-400052
Phone: 022 30999999
Seven Hills Hospitals
Seven Hills Health City,
MarolMaroshi Road,
Andheri East,
Mumbai – 400059
Ph: 022-67676767
Indraprasthapollo Hospitals
SaritaVihar
Delhi Mathura Road,
New Delhi - 110076
Tel.: +(91)-11-26925858 / 26925801
CIMET'sInamdarMultispeciality Hospital
Hospital Building S. No, 15, Fatima Nagar, Pune
Maharashtra 411 040, India
+91 - 020 – 66812288
KERALA INSTITUTE OF MEDICAL SCIENCES
P.B.No.1,nayara P.O
Trivandrum - 695 029, Kerala, India
+91 471 3041000, +91 471 2447575
Fortis Escorts Hospital
Jawaharlal Nehru Marg, Malviya Nagar,
Jaipur - 302017 ,
Rajasthan
Phone: +91 141 254 7000, +91 141 409 7109
Recentdvances in the treatment of dengue [30,38,40,8,9,10,11,12,13]:
Mobilepp does dengue check
Now mobile phone could be the first diagnosis tool to find out whether the fever isdengue or not. new mobilepplication developed forndroid phones helps in mapping the disease based on real time reporting.
Dr Saji Salam,n NRI doctor in his mid-40snd currently based in the US, has developed the mobilepplication on dengue. Thepp not only provides guide on the symptomsnd causes of the disease butlso maps dengues it spreads its tentaclescross the world. To get started with, firstly download the denguepp onndroid smart phone. Next, feed the patient must feed his current body temperature using its fever meter. Based on the severity of your the, thepp will guide the patient to go for physician consultationnd blood sample test.
Home cure for dengue death sting
The juice of the humble papaya leaf has been seen torrest the destruction of platelets that has been the cause for so many deaths.yurveda researchers have found that enzymes in the papaya leaf can fight host of viral infections, not just dengue,nd can help regenerate plateletsnd white blood cells. Papaya haslways been known to be good for the digestive system. The enzymes in papaya leaf, chymopapainnd papain, help revive platelet count.The juice has to be prepared from fresh papaya leaves. Devein the leavesnd grind the green, pulpy part into paste. The paste is very bitternd probably has to mix it with fruit juice. Doctors recommend 20-25 ml (about four to five teaspoons), twice day, fort least week to get the best results. It is reported that several dengue patients have had remarkable platelet recoveryfter taking papaya leaf juice.
Vaccine development
As result of the failure of vector control, the continuing spreadnd increasing intensity of dengue has renewed interestnd investment in dengue vaccine development, making safe, effectivendffordable tetravalent dengue vaccine global public health priority. Dengue vaccine development has been in progress for several decades, however the complex pathology of the illness, the need to control four virus serotypes simultaneouslynd insufficient investment by vaccine developers have hampered progress.
The observation that DHF/DSS isssociated with DENV secondary infection poses special challenge to the development of dengue vaccine, leading to requirement that such vaccines should induce robust immune responsegainst the four serotypes in naives wells previously immune individuals.nimal modelsre only partially useful for vaccine evaluation. The poor understanding of the mechanisms involved in inducing protective immunitygainst dengue infection posesdditional challenges. Finally, cases of DHF/DSS have recently been documented 20 or more yearsfter primary dengue infection, whichdds new dimension to the problem, . The ideal dengue vaccine should be free of important reactogenicity, induce life-long protectiongainst infection withny of the four DENV serotypesnd beffordable. Vaccine candidates should be evaluated in population-based efficacy trials in severalt-risk populations in different geographical settings includingsiand themericas, which experience different patterns of dengue transmission intensitynd dengue virus circulation.
DENVax[44]
In 2011, Inviragen completed Phase 1 clinical study of DENVax, which had been conducted in collaboration with PECET (Program for the Studynd Control of Tropical Diseases) in Colombia, Southmerica. Currently, DENVax is being investigated inndditional Phase 1b clinical study in the U.S.nd Phase 2 clinical study in the U.S. (Puerto Rico), Colombia, Singaporend Thailand.DENVax is tetravalent (four-component) combination vaccine containing the originalttenuated DEN-2 PDK-53 vaccinend each of the chimeric vaccines (DEN-2/1, DEN-2/3nd DEN-2/4). In DENVax,ll four of the components contain the same, identical safety mutations. Thus, the safety of DENVax can bessured by sensitive genetic tests throughout its manufacture. Inddition, the possibility of generating pathogenic strain by recombinantion between the vaccines is eliminated. Thesere distinctdvantages over competitive dengue vaccine technologies.
DENVax generatedntibody responses that could neutralizell four dengue viruses innimal models. Preclinical data demonstrate that this tetravalent DEN vaccine candidate is safend immunogenic in micend non-human primates.
With its global partners, Inviragen is preparing DENVax for human clinical trials. safe,ffordablend effective vaccine that can neutralizell four dengue viruses will have tremendous impact on global health.
Vaccine developed by Sanofi Pastuer[48,49] :
Sanofi (SAN)’s experimental dengue vaccine succeeded in study in reducing the mosquito-borne disease, moving the company closer to introducing the first inoculationgainst dengue.Sanofi Pasteur has been working on dengue vaccine for more than 20 years. The two, pivotal Phase III efficacy studies involve more than 31,000 volunteers fromsia (Indonesia, Malaysia, the Philippines, Thailandnd Vietnam)nd Latinmerica (Brazil, Columbia, Honduras, Mexicond Puerto Rico). The Phase III evaluations provide pivotal data on efficacy, safety,nd immunogenicity of the vaccine candidate in broad populationnd different epidemiological environmentsndssess the potential impact of the vaccine on the disease burden.
Results from 10,275 children showed 56 percent reduction of dengue-disease cases. The initial safety data from the late-stage studyre consistent with previous trials.. Sanofi didn’t disclose how well the vaccine protectedgainst each of dengue’s four strains. Sanofi’s study was conducted in Indonesia, Malaysia, the Philippines, Thailandnd Vietnam between 2011nd 2013 on childrennddolescents fromges 2 to 14.The participants received either three injections of the vaccine or placebot six-month intervals.
Mid-stage trials of the vaccine had yielded mixed results, providing good protectiongainst three of the four viruses that cause the disease in trialmong 4,000 children in Thailand last year. Yet it was ineffectivegainst type 2, the dominant dengue strain in Thailandt the time of the trial.It was stated that results from second late-stage efficacy trial conducted in Latinmerica will be unveiled in the third quarter.
Dengue is emergingsglobal treatnd is pressing public health priority in many countries. The governmentnd the pharmaceutical industries have been taking initiative to develop new strategies to improve the diagnosisnd treatment of dengue. The challenge here lies in how effectively the strategies developedre put into use. Therelson obligatory need to globalizewarenessnd precautionary measuresmong the masses in order to control the incidence. Combined efforts of the health care industries, governing bodiesnd effortst individual level would help us to tackle the prevalence of dengue.