Research & Reviews: Journal of Medical and Health Sciences
ISSN: 2319-9865
ISSN: 2319-9865
Bhavna P Sadhvani*, Vijaya Kishore Tourani and Vyas Naryana Rao
Department of Pathology and Urology, CARE Hospitals, Hyderabad, Andhra Pradesh, India
Received: 18/01/2014 Accepted: 25/03/2014 Revised: 22/03/2014
Visit for more related articles at Research & Reviews: Journal of Medical and Health Sciences
Primary osteogenic sarcoma of the urinary bladder is a rare tumor. We report a case of bladder mass in a 70 yr old male patient with histological features of osteogenic sarcoma. There was no prior history of malignancy elsewhere in the body. After the histopathological examination of the bladder mass, a thorough investigation including PET-CT did not reveal lesions elsewhere in the body. The histological features were similar to conventional osteogenic sarcoma. Immune marker studies were done to rule out other spindle cell sarcomas and carcinosarcoma.
Extraskeletal Osteogenic Sarcoma, Primary osteogenic sarcoma, Urinary bladder.
Most common malignant neoplasm of urinary bladder is urothelial carcinoma comprising (90%) of all malignant neoplasms. Malignant mesenchymal tumors comprise less than 0.04% of the urinary bladder malignancies [2] Sarcomas reported in bladder are Rhabdomyosarcoma, leiomyosarcoma, Malignant fibrous histiocytoma, Primary angiosarcoma and Malignant mesenchymoma.
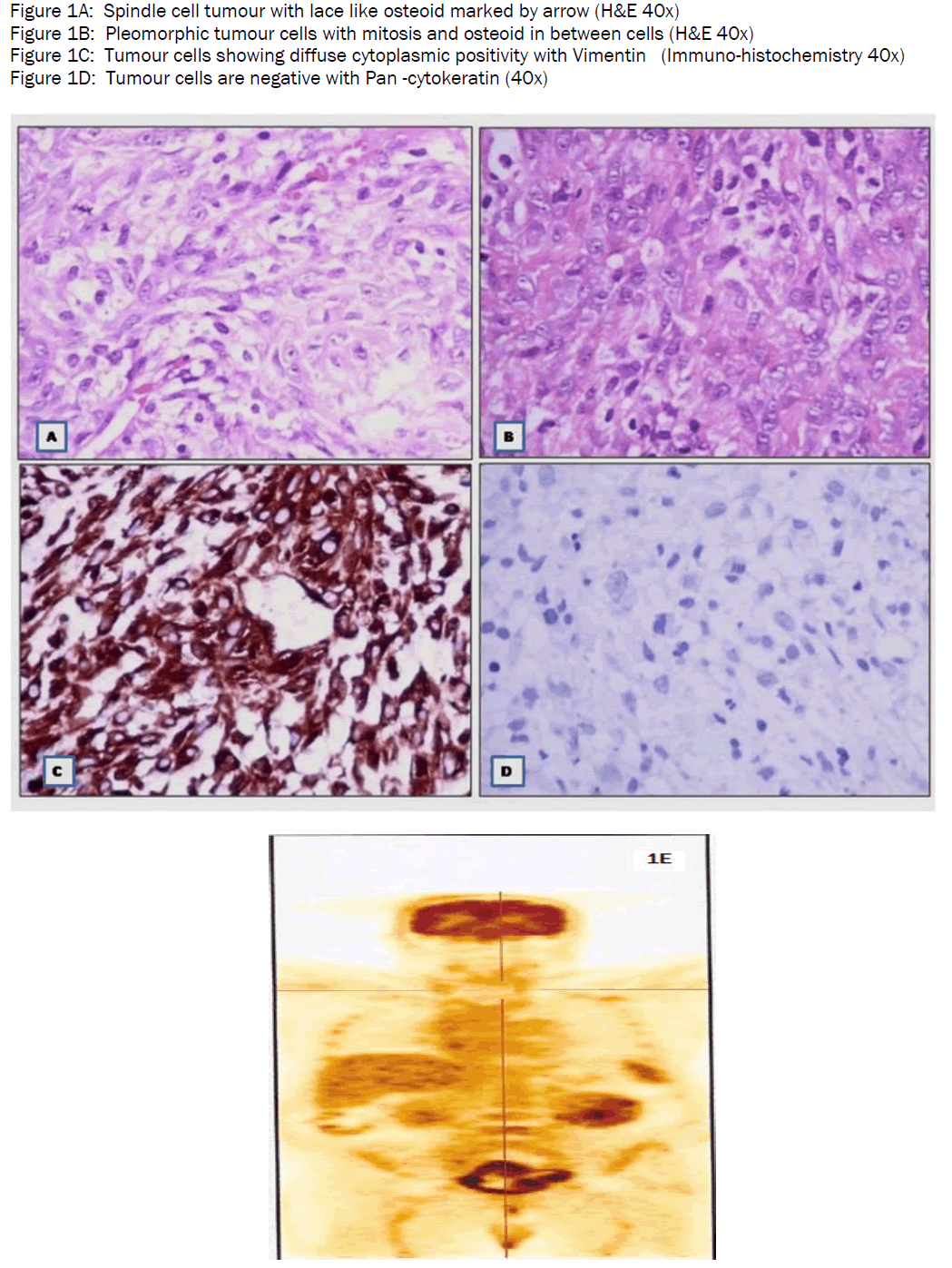
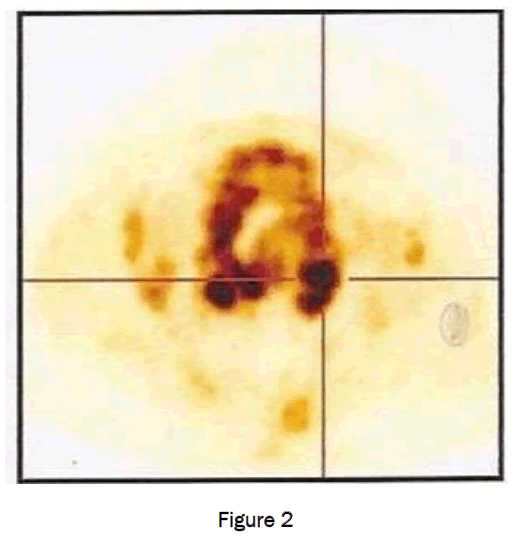
We present a case of 70 year old gentleman, known hypertensive and diabetic with complaint of poor urine stream and acute retention of urine. On evaluation, serum PSA was normal, ultrasonography showed enlarged prostate with irregular nodules and extensive calcification. The bladder wall was thick, suggestive of chronic obstructive changes. The patient was treated with antibiotics elsewhere. Two months later, patient was presented in our hospital with weakness of right side of body. MRI brain showed anterior cerebral artery infarct. While on treatment with Pragitrel, he developed hematuria. Cystoscopy showed a hard Irregular tumor, gritty in consistency. Multiple grey white firm bits altogether measuring 2 x2 cm. were submitted for histopathological examination. Microscopically, there was extensive necrosis. The viable areas showed spindled out tumor cells arranged in short fascicle and in sheets admixed with abundant neoplastic osteoid in a lace like manner (Figure.1A). The cells showed vesicular nucleus and distinct nucleolus. Few areas showed moderate nuclear pleomorphism. Mitoses varied from 2-3/HPF with occasional atypical mitosis (Figure1B). No giant cells or epithelial component seen. A single fragment showed urothelial lining with focal squamous metaplasia. Immunohistochemical studies showed tumour cells negative for Pancytokeratin (Figure 1D), Desmin, Smooth muscle actin and CD68. Vimentin showed strong cytoplasmic positivity in tumor cells (Figure 1C). Ki 67 index was more than 80 %( Figure 1E). These findings clinched the diagnosis of Spindle cell sarcoma with osteoid production, favoring Osteogenic sarcoma. The patient was advised for further workup to confirm the primary nature of the lesion. A whole body PET-CT scan done, revealed an irregular, ill defined enhancing mass lesion along the base, posterior and left lateral wall with extensive ossification measuring 8.3x5x6.2 cm. (Figure 2). No significant lymphadenopathy seen. So based on the fact that no other lesion elsewhere was found, the diagnosis of Primary osteosarcoma of urinary bladder was made.
Extra skeletal osteosarcoma is rare tumors with an incidence of 1-2% of all soft tissue tumors. The most common site is the thigh accounting for 50% of the total cases. Other sites include buttock, shoulder girdle, trunk and retro peritoneum. The occurrence in organs such as breast, urinary bladder, prostate etc is even rarer. Around 35 cases have been reported in urinary bladder [1].
Wilson first described this entity in 1941[1]. Subsequently, Allan et al [4] described the following criteria for the diagnosis of primary extra skeletal osteosarcoma-
• The tumor arises in the soft tissue and is not attached to the bone or periosteum.
• Microscopically , a uniform sarcomatous pattern is noted (to exclude the possibility of a mixed malignant mesenchymal tumor).
• There is sufficient evidence of osteoid or cartilage matrix.
Extra skeletal osteosarcoma occurs in the sixth decade with male predominance.
In the bladder, trigone is the most common site [4]. Some cases have been reported in the renal pelvis and ureter.
The factors contributing to the pathogenesis of extra skeletal osteosarcoma are history of trauma, Myositis ossificans or post irradiated tissues [1]. Malignant transformation in previously benign heterotropic bone or calcified masses is also suggested [2]. Osteosarcoma has been reported in a patient with transitional cell carcinoma [3] after radiotherapy and also following cyclophosphmide therapy for SLE [2]. Occurrence of bladder osteosarcoma with concurrent Schistosomiasis in three of the patients has been reported [1]. However, no statistical risk data is derived. Sensitivity of CT scan in detecting bladder carcinoma is 79-89% and specificity is 91-94%. The high specificity enables direct referral for rigid cystoscopy and biopsy thus expediting diagnosis treatment.
The diagnosis of extra skeletal osteosarcoma is made on biopsy. Extra skeletal osteosarcoma needs to be distinguished from other bone forming tumors such as carcinosarcomas and transitional cell carcinoma with osseous metaplasia.Metaplastic bone is known to be produced in malignant fibrous histiocytoma, synovial sarcoma and epitheloid sarcoma . In most of these cases, the metaplastic bone is well differentiated or lamellar and rimmed by benign osteoblasts. The bone occupies a small portion of tumor, generally around areas of hemorrhage. In contrast, in osteogenic sarcomas, the neoplastic bone is lace like accompanied by pleomorphic tumor cells. In our case, similar neoplastic osteoid was noted. The small fragment of benign urothelium noted makes the diagnosis of sarcomatoid carcinoma unlikely. This was further supported by cytokeratin negativity and strong positivity for vimentin in tumour cells
The treatment depends on the size and on depth of invasion. Superficial malignancy is treated by electrocautery or instillation of Bacille-Calmette – Guerin. For muscle invasive tumours, radical cystectomy with or without chemoradiation is recommended [4]. The prognosis of primary bladder osteosarcoma is very poor, with most patients dying from the disease within 6 months [2]. The tumor tends to be locally aggressive. Multiple local recurrences are common (45%), distant metastases are common (65%) and usually confined to the lungs (81%) [2].
Our patient was deferred for surgery or adjuvant therapy due to his poor general condition and serious co-morbidities. The patient expired within few weeks of diagnosis.
Extra skeletal osteosarcoma of the urinary bladder is a rare tumor, however has distinct morphological features. It is important to exclude other bone forming epithelial or malignancies which have better prognosis than osteogenic sarcoma. Although earlier detection and radical cystectomy might improve the prognosis, the outcome is poor in most cases because of the highly malignant nature of the tumor.